The forum was opened by Prof Brendan Murphy.
His main message was the government does not believe that chronic diseases can be caused by chronic infections. This theme resonated through the forum.
The government acknowledges that rickettsia can be transmitted by ticks so ticks can transmit pathogens. Bartonella as a tick borne infection was not acknowledged even though there have been scientific publications about this.
There were more patient stories. The audience were mostly from minor patient advocate groups, who themselves were patients. There had been ample patient stories in the Senate Committee submission so why more patient stories?
The aim of the forum was to discuss the way forward with multidisciplinary teams (MDT) and insufficient time was allowed for this main topic
NHMRC presented the process of grant application for the DSCATT TCR for the $3 mill allocated by the Hon Health Minister Greg Hunt.
Why was there only $3 million allocated for TBD research? In real research terms $3 million is a meagre amount.
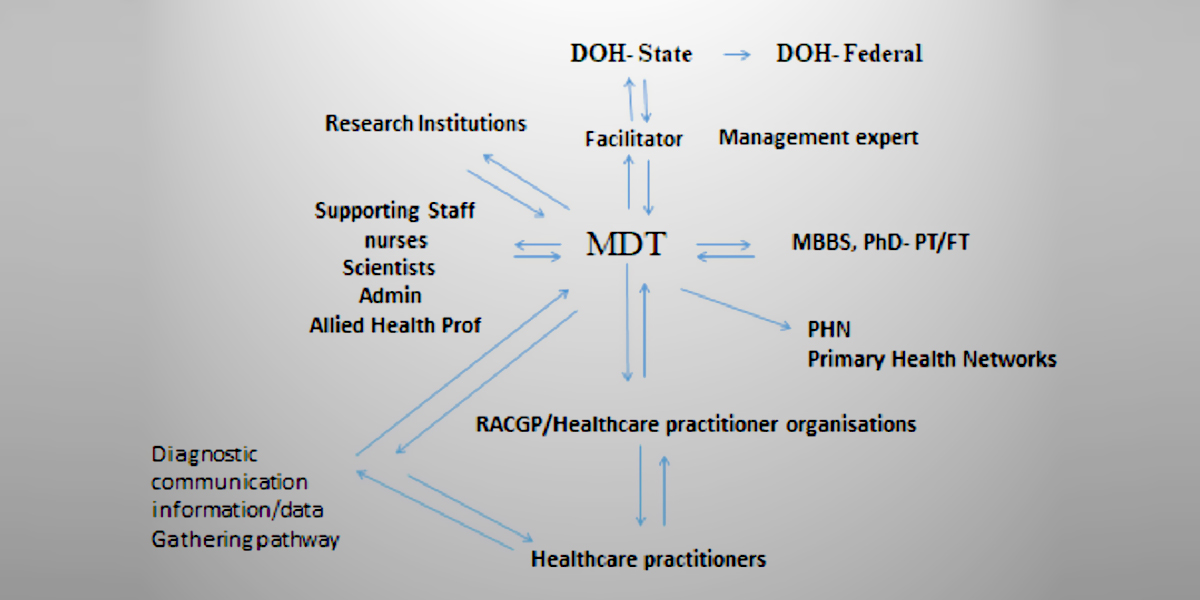
For MDT there were two presentations, one by KMF addressing the way forward with multidisciplinary teams. The model presented was for the current situation designed to allow better diagnosis of tick borne diseases without discrimination/prejudice of Lyme disease. The model below allows for collection of data for acute and chronically ill TBD patients. It also ensures that the MDT is composed of broad minded young registrars who are undertaking their PhD, or have a PhD so that exploratory diagnosis can be done without the restraints of mainstream practices. This model also allows for source patients for clinical research. The MDT model can behave like a mini CDC of USA. It can educate GPs in the front line via RACGP and other professional groups.
With increased education there can be better diagnosis of patients with tick borne diseases both acute and chronic. Once a GP suspects a patient may have TB infections they can liaise with the MDT professionals to enable better exploration of diagnosis. Improved diagnosis also translates better treatment. This can only happen if the MDT professionals are well supported by the latest developments in the TBD field, which includes possible diagnosis of relapsing fever and reptilian Borrelia and Babesia, Bartonella, Anaplasma, Ehrlichia and others, without Lyme prejudice.
KMF model can be implemented within a year within the current public health system.
This will enable those who are ill and can’t afford expensive medical fees or overseas treatment clinics to be cared for. They can be treated as appropriate for Australian tick borne infections in Australia.
The other model presented by LDAA advocated uniting with the chronic fatigue syndrome (CFS) and Biotoxin groups and use the increased number of patients to participate in a biomarker trial. This model concurs with the view of the government that chronic diseases cannot be due to infection. Biomarkers represent the host response to disease. Most biomarkers are immune system communication tools, ie: cytokines, interleukins, membrane markers etc. These all represent the immune response and usually the immune system responds to disease by generalized inflammation. It can’t afford to provide a unique respond to each disease. The uniqueness of the immune system arises from it ability to lay down pathogen memory and synthesis of specific antibodies. It is not conducive for evolution to respond to each disease in unique fashion.
With multinational testing subgroups of patients can be created but it does not address the cause/reason why markers are increased or decreased.
This model preclude the use of antibiotics for chronic tick borne diseases patients. It provides an opportunity to develop medications which are either agonists or antagonists or ways of supplementing missing biomarkers. It is a palliative way of addressing disease. It is does not provide a “cure” option.
Dr M McManus



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave A Comment
You must be logged in to post a comment.